We have this notion – or perhaps a false hope – that excision surgery is going to miraculously take away all the pain and suffering leading up to this day. And, while excision is the gold standard of diagnosing and treating endometriosis, it is always good to be prepared for lingering AND new symptoms that appear after the body has settled post-surgery. I am going to do a much more thorough post on central sensitization as I think it is such a huge component of recovery and realization. More on that later. But for now, I wanted to discuss something very important in terms of listening to your body and accepting that it is unique.
I sit here 6 weeks post op, wondering why this menstrual period – minus the bleeding since I ‘skip my periods’ – is so mentally and physically exhausting. One of the main symptoms that you know all too well is the menstrual pain (dysmenorrhea). Dysmenorrhea as a blanket term refers to the excruciating pelvic pain accompanied by menstruation – aka period cramps. We all know it. It’s one of the first signs we as #endowarriors experienced in those early years to foreshadow the inevitable diagnosis of endometriosis. So why then, after an extensive excision of endometrial lesions and adhesions I am yet again experiencing dysmenorrhea?
I did some research as I always do, and discovered that dysmenorrhea has been classified as primary and secondary dysmenorrhea. Puzzled how I never knew this before, I continued to read.
According to ACOG (and many other citations) “Primary Dysmenorrhea is defined as painful menstruation in the absence of pelvic pathology”. Or put another way,
Primary Dysmenorrhea is defined as cramping pain in the lower abdomen occurring just before or during menstruation, in the absence of other diseases such as endometriosis.
Dr. Andrew Coco, Lancaster General Hospital
Women who present with primary dysmenorrhea also express sharp, intermittent spasms typically in the suprapubic area, with pain radiating down their lower back and legs. We know that during menstruation, the shedding of the endometrial lining releases prostaglandins – more specifically PGF2-alpha. “PGF2a stimulates myometrial contractions, ischemia and sensitization of nerve endings” according to Coco. In turn, women with primary dysmenorrhea have higher levels of this PGF2a in their menstrual fluid. The research I have read all claim that women with primary dysmenorrhea experience significant relief with the use of NSAIDS which inhibit prostaglandin production and release. For those who do not experience relief – like so many of us – clinically this raises the question whether the patient has secondary dysmenorrhea – menstrual cramping in the presence of pathology.
As we know from personal experience, if secondary dysmenorrhea is speculated, a hierarchy of tests are done to determine if the patient should have a laparoscopic procedure done to diagnose the patient and excise the endometrial tissue. The most common cause of secondary dysmenorrhea is endometriosis. Other causes of secondary dysmenorrhea include (in no order, adopted from ACOG):
- congenital obstruction mullerian malformations
- cervical stenosis
- ovarian cysts
- uterine polyps
- uterine leiomyomata
- adenomyosis
- pelvic inflammatory disease
- pelvic adhesions
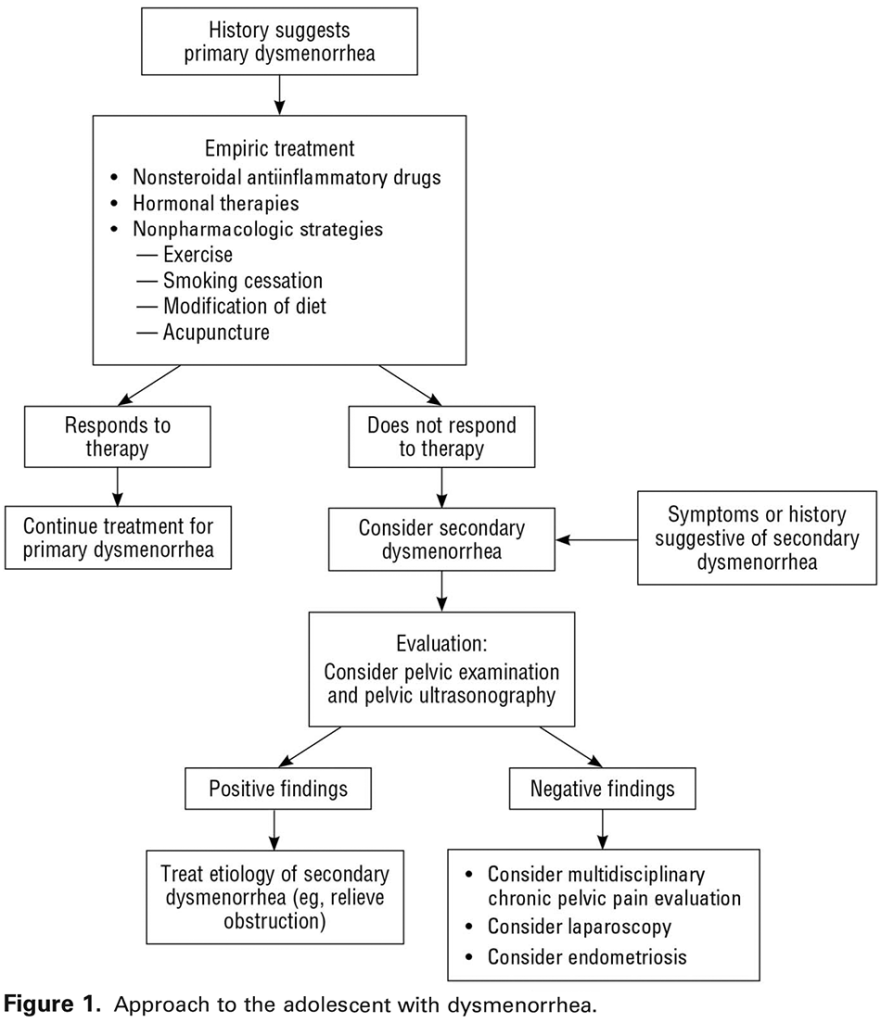
Figure 1 above shows the fairly simplistic outline on how to discern primary vs secondary dysmenorrhea. Note that in the chain of events leading to a conclusion of endometriosis, birth control pills are often prescribed to mitigate symptoms of pain and cramping while discovery is still happening. Birth control works in a different way than NSAIDS. First, the birth control is used to reduce the menstruation – or rather the volume of fluid being released during menstruation. Second, it suppresses ovulation if the patient is skipping the 7 day sugar pills and continuing straight through. However, birth control should NOT be used as a bandaid and should be part of a much larger discussion.
So back to my pondering. If then, the endometriosis. or the pathology classifying secondary dysmenorrhea is removed, can one then resume primary dysmenorrhea? Say, at the age of 14, before endometrial lesions formed and I was having primary dysmenorrhea (big assumption here) does one resume primary dysmenorrhea post excision? Im still looking to find out as this would clinically mean I would respond to NSAIDS and I would continue to have ‘bad periods’ even in the absence of pathology like endometriosis. Big questions! Leave your comments – I love reading them!
References:
